

WORLD TB DAY – 2023 (PROVINCIAL TB CONTROL PROGRAM PUNJAB)
July 10, 2026
Drug-Resistant Tuberculosis in Punjab: How a 27-Site Network Is Rewriting the Rules of TB Treatment in Pakistan
Somewhere in Punjab today, a patient will be told the words no one wants to hear: “the usual TB medicine isn’t working for you.” A generation ago, that sentence often meant a treatment journey stretching past two years, a fistful of daily injections, and odds that weren’t in the patient’s favour. Today, in 2024, that same patient can be started on an all-oral, 6-month cure — and can walk into one of 27 dedicated Drug-Resistant TB sites across Punjab to get it, free of cost.
This is the story of how Drug-Resistant Tuberculosis (DR-TB) is being managed in Pakistan, why Punjab’s response matters on a global scale, and what every patient, family member, and healthcare worker needs to know about the province’s expanding treatment network.
Why Drug-Resistant TB Is a National Emergency, Not Just a Medical Term
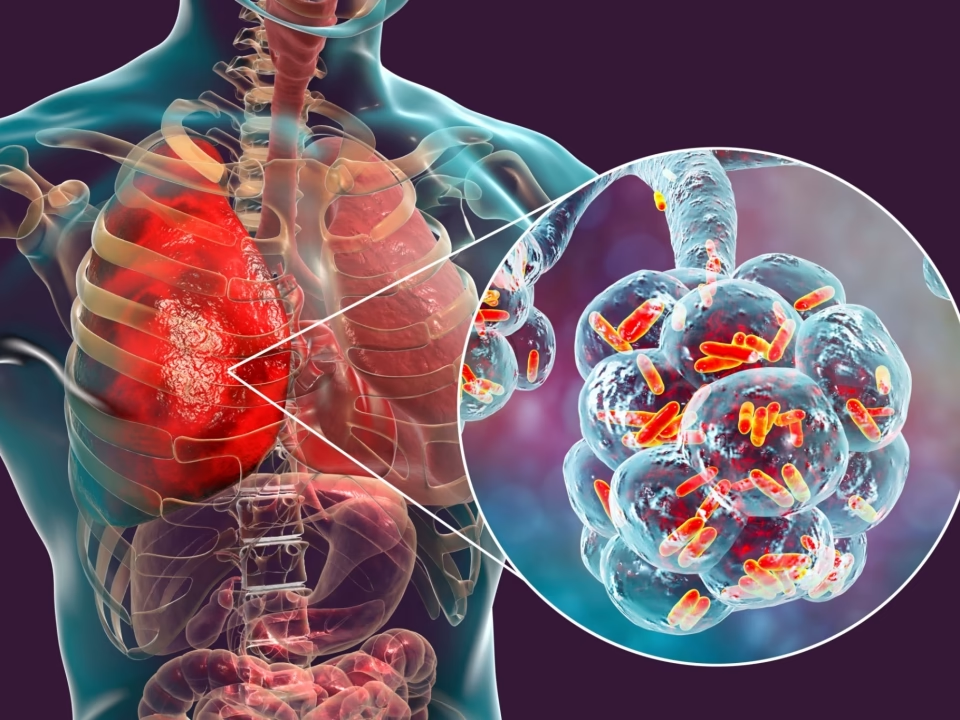
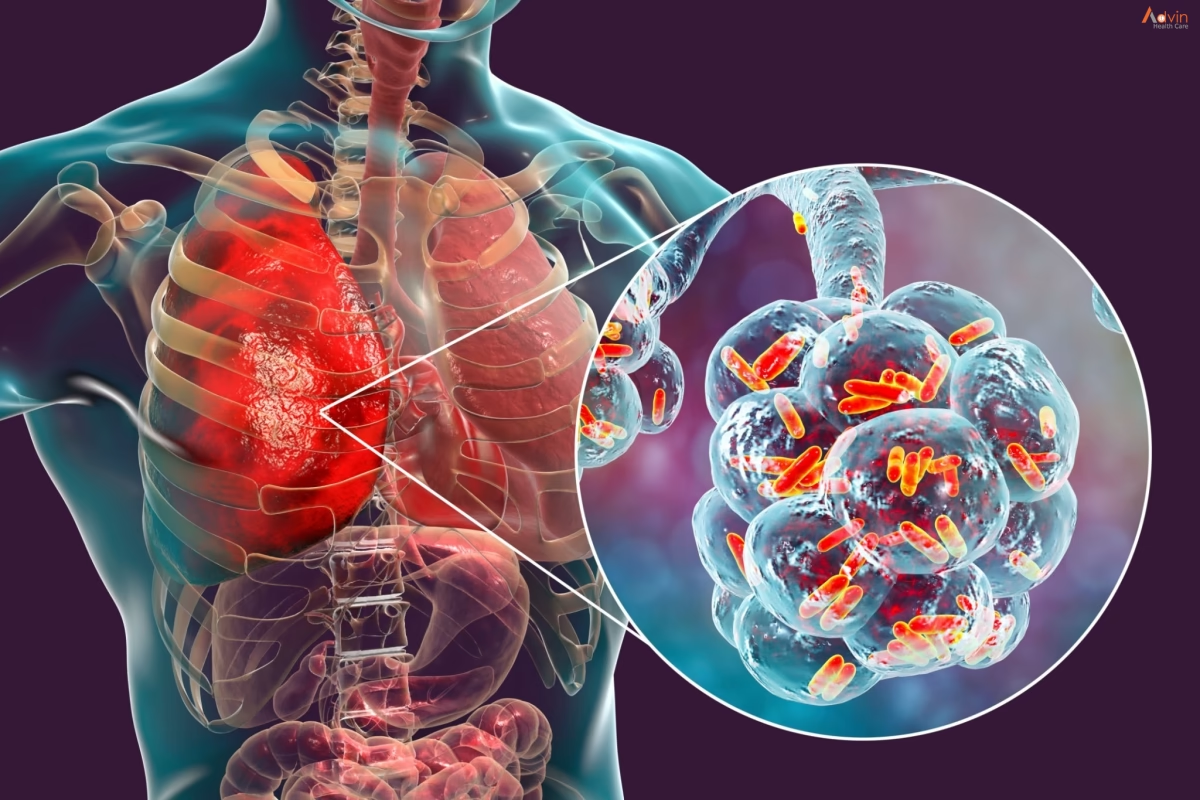
Tuberculosis has treatable, curable forms — but when the bacteria that cause it mutate and stop responding to standard first-line drugs, the disease becomes something far tougher to fight: Drug-Resistant Tuberculosis, commonly shortened to DR-TB or MDR-TB (Multidrug-Resistant TB).
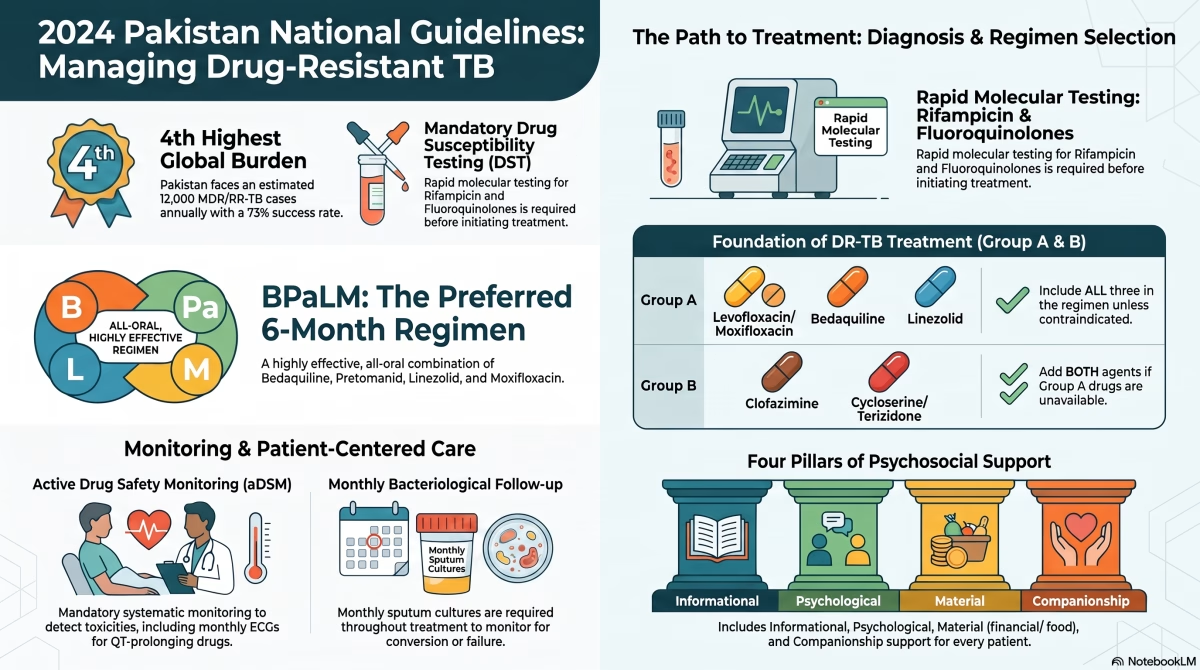
The numbers explain why this is a national priority. According to the Global TB Report, Pakistan ranks 4th among the world’s 20 high MDR/RR-TB burden countries, with an estimated 12,000 new MDR/RR-TB cases emerging every year and an incidence rate of roughly 5.4 per 100,000 people. Drug resistance is present in an estimated 2.3% of new TB cases and a striking 4.6% of previously treated cases — and of those resistant cases, nearly 40% already show signs of Pre-XDR TB, meaning the bacteria are becoming resistant to even more drug classes.
The encouraging part of this picture: treatment success rates have climbed from 64% (2015–17) to 73% (2018–19), largely because of the introduction of newer, more powerful drugs like Bedaquiline. That progress is exactly what Punjab’s expanding DR-TB network is built to accelerate.
Understanding the Different Faces of Drug Resistance
Not all “resistant” TB is the same, and the distinction matters enormously for treatment decisions. The WHO classification — followed by Pakistan’s National TB Programme — breaks it down as follows:
- HR-TB (Isoniazid-Resistant TB): Resistant to Isoniazid but still responds to Rifampicin.
- RR-TB (Rifampicin-Resistant TB): Resistant to Rifampicin, the cornerstone first-line drug — regardless of Isoniazid status.
- MDR-TB (Multidrug-Resistant TB): Resistant to both Rifampicin AND Isoniazid, the two most powerful first-line drugs.
- Pre-XDR-TB: RR-TB plus resistance to a Fluoroquinolone (Levofloxacin or Moxifloxacin).
- XDR-TB (Extensively Drug-Resistant TB): RR-TB plus resistance to a Fluoroquinolone AND at least one Group A drug such as Bedaquiline or Linezolid.
This resistance doesn’t appear out of nowhere. It develops through genetic mutations — changes in genes like katG, inhA (linked to Isoniazid resistance), rpoB (Rifampicin resistance), and gyrA (Fluoroquinolone resistance) — often triggered by incomplete treatment courses, poor adherence, substandard drug quality, or inadequate dosing. It can also spread directly from person to person through primary transmission of an already-resistant strain. Understanding this mechanism is precisely why Punjab’s programme places such heavy emphasis on early, accurate diagnosis before treatment ever begins.
Diagnosis First: Why Testing Cannot Be Skipped
No DR-TB regimen should ever be started blind. Drug Susceptibility Testing (DST) is the non-negotiable first step, and Punjab’s laboratory network is built around rapid molecular tools that can detect resistance to Rifampicin, Isoniazid, and Fluoroquinolones — with the newer Xpert MTB/XDR test returning results in under 90 minutes.
There are still gaps, of course. Rapid molecular testing isn’t yet available for every drug — Ethambutol, Bedaquiline, Clofazimine, Linezolid, Pretomanid, and Delamanid still rely on slower, culture-based (phenotypic) testing, which remains especially critical for detecting Fluoroquinolone resistance given how prevalent it already is in Pakistan. On the horizon, the WHO’s newly recommended targeted Next Generation Sequencing (tNGS) promises to test for resistance to multiple anti-TB drugs simultaneously, a genuine leap forward for programmes like Punjab’s.
The Treatment Itself: From Two Years of Injections to Six Months of Tablets
This is where the story of DR-TB care has changed the most. Pakistan’s National TB Programme, aligned with WHO’s latest guidance, now offers three main pathways depending on a patient’s resistance profile:
1. BPaLM — The Preferred 6-Month, All-Oral Regimen
For most patients with confirmed MDR/RR-TB where Fluoroquinolone susceptibility is presumed or confirmed, BPaLM is now the gold standard: Bedaquiline, Papretomanid, Linezolid, and Moxifloxacin, taken entirely by mouth for just six months. Where Fluoroquinolone resistance is confirmed, the regimen drops the “M” and becomes BPaL.
Each component plays a distinct, deliberate role:
- Bedaquiline — a diarylquinoline that inhibits the TB bacteria’s energy production (ATP synthase)
- Pretomanid — a nitroimidazole active against both actively multiplying and dormant TB bacteria
- Linezolid — an oxazolidinone that blocks bacterial protein synthesis
- Moxifloxacin — a Fluoroquinolone, omitted only where resistance is confirmed
2. The 9-Month All-Oral Regimen
An alternative for patients where Fluoroquinolone resistance has been excluded, combining Bedaquiline (used for 6 months) with Levofloxacin/Moxifloxacin, Clofazimine, Pyrazinamide, Ethambutol, and either Ethionamide or a 2-month course of Linezolid.
3. The Longer Individualized Regimen (18+ Months)
Reserved for patients who aren’t eligible for the shorter regimens, those with confirmed XDR-TB, or those who cannot tolerate key drugs. These regimens are custom-built using WHO’s hierarchical drug grouping — Group A (Levofloxacin/Moxifloxacin, Bedaquiline, Linezolid), Group B (Clofazimine, Cycloserine/Terizidone), and Group C (Ethambutol, Delamanid, Pyrazinamide, carbapenems, Amikacin, Ethionamide, PAS) — added in that order of priority.
Safety Isn’t an Afterthought — It’s Built Into Every Step
Powerful drugs demand equally powerful safety monitoring, and this is where Punjab’s programme leans on Active Drug Safety Monitoring (aDSM) — a mandatory, systematic surveillance protocol for every single patient on an MDR/RR-TB regimen. This includes:
- ECG monitoring for drugs known to prolong the QT interval (Bedaquiline, Delamanid, Moxifloxacin, Clofazimine)
- Blood counts and liver function tests, especially important for patients on Linezolid, where prolonged use can cause pancytopenia or lactic acidosis
- Visual and neurological checks for drugs linked to optic or peripheral neuropathy, such as high-dose Isoniazid, Cycloserine, and Ethambutol
- Uric acid and liver monitoring for Pyrazinamide and Ethambutol
Alongside clinical safety, treatment response is tracked through monthly sputum smear microscopy and culture, with sputum conversion — two consecutive negative cultures — used as the key marker of progress, and repeat DST ordered if a culture stays positive or reverts after initially turning negative.

Treating the Whole Person, Not Just the Infection
One of the most human elements of Punjab’s DR-TB programme is its recognition that a 6-to-18-month treatment journey is as much a psychological and financial challenge as a clinical one. Psychosocial support is written into the programme as a mandatory component, covering four pillars:
- Informational support — helping patients understand their medication, expected side effects, and what “success” actually looks like
- Psychological support — building self-esteem and trust to help patients push through a demanding treatment course
- Material support — financial grants, food assistance, and travel reimbursement to offset the direct and indirect costs of TB care
- Companionship support — ensuring patients never feel isolated, but instead feel anchored to a support network throughout treatment
Punjab’s DR-TB Network: 27 Sites, One Mission
Perhaps the clearest sign of how seriously Punjab is treating this challenge is the sheer scale of its dedicated infrastructure. The province now operates 27 specialized DR-TB facilities, split across two tiers of care:
13 PMDT (Programmatic Management of Drug-Resistant TB) Sites, managed jointly by the Provincial TB Control Programme (PTP) Punjab and the Association for Social Development (ASD):
| Managed By | Site Name |
|---|---|
| PTP Punjab | Gulab Devi Hospital, Lahore |
| PTP Punjab | DHQ Gujranwala |
| PTP Punjab | Military Hospital, Rawalpindi |
| PTP Punjab/ASD | Rawalpindi Leprosy Hospital |
| PTP Punjab/ASD | Samli Sanatorium, Murree |
| PTP Punjab/ASD | Jinnah Hospital, Lahore |
| PTP Punjab/ASD | Mayo Hospital, Lahore |
| PTP Punjab/ASD | AIMH Hospital, Sialkot |
| PTP Punjab/ASD | DHQ Teaching Hospital, Sargodha |
| PTP Punjab/ASD | DHQ Hospital, Faisalabad |
| PTP Punjab/ASD | Nishtar Hospital, Multan |
| ASD/PTP Punjab | SZ Hospital, Rahim Yar Khan |
| ASD/PTP Punjab | BVH, Bahawalpur |
14 DR-TB Clinics, extending specialized care into district-level facilities under PTP and ASD management:
| Managed By | Site Name |
|---|---|
| PTP | DHQ Vehari |
| PTP | DHQ Chakwal |
| PTP | DHQ D.G. Khan |
| PTP | DHQ Khanewal |
| PTP | DHQ M.B. Din |
| PTP | DHQ Jhang |
| PTP | DHQ Lodhran |
| PTP | DHQ Mianwali |
| PTP | DHQ Layyah |
| PTP | DHQ Bahawalnagar |
| PTP | DHQ Kasur |
| ASD | DHQ Attock |
| ASD | DHQ Okara |
| ASD | DHQ Sheikhupura |
This dual-tier structure means that regardless of where a patient in Punjab lives — from Rawalpindi in the north to Rahim Yar Khan in the south — there is a dedicated, government-backed DR-TB facility within reach, offering free diagnosis, free medication, and structured clinical monitoring throughout the treatment course.
The Bigger Picture: What This Means for Punjab
Seven takeaways stand out from where Punjab’s DR-TB response stands today:
- Pakistan’s 4th-place global ranking for MDR/RR-TB burden makes early diagnosis and prompt treatment a genuine national priority, not a bureaucratic checkbox.
- BPaLM is now the preferred, WHO-backed, 6-month all-oral cure for most MDR/RR-TB patients in Pakistan.
- Drug Susceptibility Testing — especially for Rifampicin, Isoniazid, and Fluoroquinolones — is mandatory before any DR-TB treatment begins.
- All three Group A drugs (Levofloxacin/Moxifloxacin, Bedaquiline, Linezolid) should feature in every regimen unless medically contraindicated.
- Active Drug Safety Monitoring is mandatory for every patient on an MDR/RR-TB regimen, with ECG monitoring non-negotiable for QT-prolonging drugs.
- Psychosocial support — informational, emotional, material, and companionship — is treated as a core programmatic pillar, not an optional extra.
- A 27-site network across Punjab means specialized DR-TB care is no longer confined to a handful of tertiary hospitals — it is now a genuinely province-wide service.
Final Word
Drug-Resistant Tuberculosis is still one of the toughest challenges in Pakistan’s public health landscape — but the gap between “resistant” and “incurable” has never been narrower. With shorter, all-oral regimens, rigorous safety monitoring, dedicated psychosocial care, and a growing network of 27 specialized sites across Punjab, patients today have a real, evidence-based path back to health.
If you or someone you know has been diagnosed with drug-resistant TB, the nearest PMDT site or DR-TB clinic listed above is the place to start — treatment is free, confidential, and backed by Pakistan’s National TB Programme guidelines.
This article is based on the Pakistan National TB Case Management Guidelines 2024 and the Provincial TB Control Programme (PTP) Punjab’s current network of DR-TB treatment sites.

{kind=link}
{kind=link}